
Moving to remote autism diagnosis during the COVID-19 pandemic
Published on 24 May 2022
Author: Dr Rob Ogley, Dr Conor James Davidson, Dr Alwyn Kam
Dr Rob Ogley, Dr Conor Davidson and Dr Alwyn Kam from the Leeds Autism Diagnostic Service, discuss the move to remote autism diagnostic assessments for adults during the COVID-19 pandemic. The article also explores service user feedback and the lessons learned.
Leeds Autism Diagnostic Service is an autism specialist service for adults and is based in the city of Leeds, United Kingdom. We are an all-ability service, seeing service users of any intellectual ability (IQ). We accept self-referrals as well as referrals from health and social care professionals. The assessment process typically involves three stages:
- a background history,
- a developmental history from a parent/carer
- a clinical decision meeting (CDM) including elements based on the Autism Diagnostic Observation Schedule (ADOS).
Transitioning to remote assessment
In response to the COVID-19 pandemic, LADS moved to remote consultations. Initially, the first two information-gathering stages were changed to telephone appointments. As the CDM includes ADOS-based interactive tasks and assessment of non-verbal communication, it was carried out over videocall.
The service selected Zoom as its preferred videocall platform, as this has a ‘waiting room’ feature needed to accommodate private clinician discussions during appointments.
The ADOS involves a variety of interactive visual tasks. Many of these converted well to the ‘screen sharing’ function, however some required physical items (like the ‘puzzle task’) and were therefore left out. ADOS has not been validated for online diagnosis so we used it to gather clinical information and structure the CDM. We were able to clinically diagnose on the basis of the information gathered from all the appointments.
In May 2020 our service began to use videocalls as standard. 133 videocall CDM’s were completed up to 31st December 2020, with only ten being conducted face-to-face (FTF). The most common reasons for preferring FTF were difficulties using technology and risk/mental health issues (such as delusions that prevent engagement with videocalls).
Diagnostic rates
We compared non-attendance and diagnostic rates (in other words the proportion of CDM’s resulting in autism diagnosis) for videocalls in 2020 versus FTF in 2019-2020. The videocalls showed a diagnosis rate (excluding non-attenders) of 72.9% , with 2.9% not attending (three of these due to technical difficulties). For FTF in the figures were 64.9% (n 200/308) and 6.7% not attending(n 22/330). Therefore there was no statistically significant change in diagnostic rates following a move to remote assessment.
Difficulties with videocalls
There were some difficulties with using videocalls, including issues with:
- poor bandwidth;
- small screens making the picture tasks difficult;
- noisy/chaotic households;
- privacy concerns.
We found it more difficult at times to assess non-verbal communication such as gestures, even when the whole upper body was visible.
Service User feedback
Figures 1 and 2 show preferences relating to FTF, telephone and videocall appointments from 63 service user satisfaction questionnaires, filled out between July 2020 and February 2021.
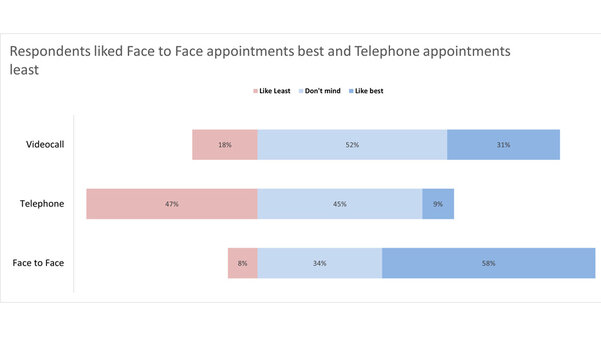
Figure 1: service user preferences between videocall, telephone and FTF

Figure 2: Service user attitude to videocalls
Key themes from comments were (in descending order of frequency):-
- videocalls provide a good experience;
- videocalls offer choice;
- videocalls are good for those with transport issues;
- barriers to videocall use include technology issues and the distraction of seeing yourself;
- waiting for the Zoom appointment link just before the appointment is stressful.
Service user comments:
“I would always prefer face to face as its personal but videocalls are the next best thing.”
“the video call helped as it took some of the apprehension about interacting with the assessors out of the situation as they weren't physically there, I didn't have to worry about eye contact and I felt more comfortable being in my own environment.”
Advice for doing successful remote assessments
Based on what was learnt, the team put together a guide to remote autism assessments. We have shared some of it here.
Preparation
- Send the videocall link before the day of appointment.
- Recommend using a tablet or computer (larger screen and hands free).
- Advise where to put the device so face and upper body are visible
- Advise being in a quiet room, free from interruptions
Pre-meeting
- Before the appointment, allow time for clinicians to discuss the case and agree specific roles - for example, who is leading the meeting and who is taking notes.
- Consider whether adaptations/reasonable adjustments are needed, such as changing the order of tasks or having more breaks.
Connecting
- Check audio/video for all participants and ensure each person is visible and audible.
- Confirm each person’s identity (even if they are off camera).
- Check where the service user is calling from, and confirm a telephone number should the call cut off.
- Ensure the service user has privacy.
Assessment
- Explain the purpose, duration and structure of the meeting including breaks.
- Explain that the service user will be placed in the virtual waiting room during breaks to allow privacy for them and the clinicians.
- Wait for the service user to leave the meeting before ending the call to ensure they do not feel they have been ‘cut off’.
Discussion
The Covid pandemic has had a huge impact on healthcare and services have been forced to change at a rapid pace. There are some potential advantages with videocall autism assessment, including convenience, reduced travel and service users feeling more comfortable in their homes rather than visiting a clinic.
Research so far suggests that the diagnostic accuracy of remote assessment is comparable to FTF (Kuhl-Meltzoff Stavropoulos et al., 2022). Although ADOS (and most autism tools) are not validated for remote use, new tools are being developed specifically for videocall, such as the BOSA (Brief Observation of Symptoms of Autism).
There are also challenges associated with videocalls but despite these it seems videocall assessment of autism remains widespread. Some services now only offer assessments online. Our feedback found 82% of respondents either preferred or did not mind remote appointments, with 62% wanting the option to be extended beyond the pandemic. In light of this LADS has retained videocall assessments for the foreseeable future.


